
Blocked Leg Arteries: Can Angioplasty Help You Avoid Amputation?
Introduction: When Blocked Arteries Put Your Legs and Your Life at Risk
Leg pain that comes on during walking and disappears with rest. A foot wound that refuses to heal. A toe that has turned dark and painful without any injury. These are not minor inconveniences they are warning signals from arteries that are narrowing, hardening, and slowly losing the ability to deliver life-sustaining blood to your legs and feet.
Peripheral artery disease (PAD) affects millions of people worldwide. In its early stages, it is manageable. In its advanced stages, it is limb-threatening. The critical question for patients and their families is this: does treatment have to mean major surgery or amputation? For a growing number of patients, the answer is neither. Modern angioplasty and endovascular techniques are offering a minimally invasive route to restored blood flow, healed wounds, and preserved limbs.
What Happens When the Arteries in Your Legs Get Blocked?
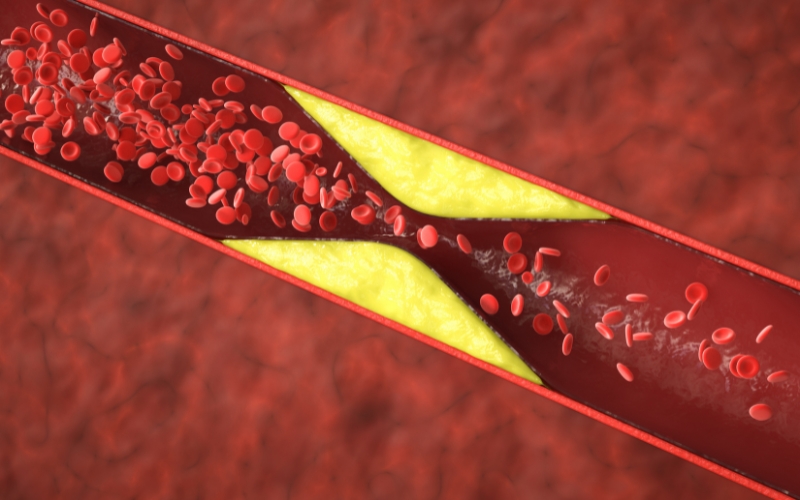
Your leg arteries carry oxygen-rich blood from the heart to the muscles, skin, nerves, and tissues of the lower limbs. When these arteries become narrowed or blocked most commonly by a build-up of fatty plaque along the artery wall blood flow is progressively reduced. At first, the muscles complain only during exertion. Over time, even resting tissue cannot receive enough oxygen to survive. The result, if left untreated, can be non-healing ulcers, gangrene, and ultimately amputation.
Why Peripheral Artery Disease Is More Dangerous Than Most People Realise
PAD is significantly underdiagnosed. Many patients attribute their leg pain to ageing, arthritis, or general fitness and never seek evaluation. Yet PAD is not merely a local leg problem it is a systemic marker of cardiovascular disease. People with PAD have a markedly elevated risk of heart attack and stroke. Identifying and treating PAD early protects not just the limb it protects the heart and brain as well.
Claudication vs Critical Limb Ischemia - Understanding the Difference
What Is Claudication? The Warning Sign You Should Never Walk Off
Claudication is the earliest and most recognisable symptom of significant arterial blockage in the leg. It presents as cramping, aching, or heaviness in the calf, thigh, or buttock that reliably appears after walking a certain distance and resolves completely within a few minutes of rest. The distance a person can walk before symptoms appear the claudication distance shortens as the disease progresses.
Claudication is your arteries telling you that blood supply is insufficient for active muscle demand. It is not something to walk through and ignore. It is a clinical sign that requires evaluation, risk factor modification, and in many cases, intervention before the disease advances to a more dangerous stage.
Critical Limb Ischemia When Blocked Arteries Become a Limb-Threatening Emergency
Critical limb ischemia (CLI) is the most severe form of PAD. It occurs when arterial blockage is so advanced that blood flow is insufficient even at rest. The hallmarks of CLI are rest pain typically burning pain in the foot at night, relieved by hanging the leg off the bed and tissue loss in the form of non-healing ulcers or gangrene. CLI is a vascular emergency. Without prompt restoration of blood flow, the risk of major amputation within twelve months is extremely high.
How Doctors Classify the Severity of Peripheral Artery Disease
Vascular specialists use two main classification systems the Fontaine Classification and the Rutherford Categories to grade the severity of PAD from asymptomatic arterial narrowing through to major tissue loss. These classifications guide treatment urgency and help determine whether lifestyle modification, medication, endovascular intervention, surgical bypass, or urgent amputation is the most appropriate course of action.
Who Is at Risk? The Risk Factors Behind Blocked Leg Arteries?
Diabetes, Smoking, and High Blood Pressure The Three Biggest Contributors
Certain risk factors dramatically accelerate the development of PAD and increase the likelihood of progression to critical limb ischemia:
- Smoking – The single most powerful modifiable risk factor for PAD. Smokers develop PAD a decade earlier than non-smokers and progress to CLI at a significantly higher rate
- Diabetes – Damages both large and small blood vessels, impairs wound healing, and causes peripheral neuropathy that masks early warning symptoms
- High blood pressure – Accelerates plaque formation and arterial wall damage throughout the vascular system
Age, Cholesterol, and Lifestyle Factors That Accelerate Arterial Blockage
PAD becomes significantly more common after the age of 50, and risk rises steeply with each decade. High LDL cholesterol drives plaque accumulation inside artery walls. Obesity, physical inactivity, and a diet high in saturated fat and refined carbohydrates all contribute to the metabolic environment in which arterial disease flourishes. Kidney disease and a history of heart disease or stroke are additional independent risk factors.
Why Some People Develop Critical Limb Ischemia With No Prior Warning?
A significant proportion of CLI patients report little or no prior claudication. This is particularly common in diabetic patients, whose peripheral neuropathy masks the pain signals that would normally prompt them to seek help. By the time a non-healing foot wound or darkened toe brings them to a vascular clinic, the arterial disease may already be at an advanced stage underscoring why regular vascular screening is important in high-risk individuals.
Modern Endovascular Treatments What Is Available Today:
From Open Bypass Surgery to Catheter-Based Intervention - How Treatment Has Evolved
Twenty years ago, restoring blood flow to a severely blocked leg artery almost always meant open bypass surgery a major operation redirecting blood around the blockage through a graft taken from another vein or made from synthetic material. While bypass surgery remains an important tool, the majority of patients with PAD can now be treated with endovascular techniques catheter-based procedures performed through a small puncture in the groin, wrist, or foot, guided by real-time X-ray imaging.
Angioplasty Explained Opening Blocked Arteries From the Inside
Balloon angioplasty is the foundation of endovascular PAD treatment. A thin catheter is guided through the arterial system to the site of blockage under fluoroscopic guidance. A small balloon at the catheter tip is then inflated precisely at the narrowing, compressing the plaque against the artery wall and restoring the vessel’s internal diameter. Blood flow is re-established immediately. The access point a single puncture is closed with a small device or manual pressure, requiring no stitches.
Who Is a Candidate for Endovascular Treatment?
Most patients with symptomatic PAD from claudication through to critical limb ischemia are candidates for endovascular treatment, provided their arterial anatomy is suitable. Assessment includes clinical examination, ankle-brachial index (ABI) measurement, duplex ultrasound, and in most cases CT angiography to map the precise location, extent, and characteristics of the blockages. The results of this imaging guide the choice of technique and help set realistic expectations for outcomes.
Drug-Coated Balloons, Stents, and Atherectomy The Tools of Modern Vascular Care:
Drug-Coated Balloons Keeping Arteries Open Longer After Angioplasty
One of the most significant advances in PAD treatment over the past decade has been the development of drug-coated balloons (DCBs). Standard balloon angioplasty carries a risk of restenosis the artery re-narrowing as the vessel wall heals. Drug-coated balloons are coated with an antiproliferative agent most commonly paclitaxel that is delivered directly into the artery wall during inflation, suppressing the cellular response that causes re-narrowing. Clinical trials have consistently demonstrated superior patency rates with DCBs compared to standard balloons in the superficial femoral and popliteal arteries.
Bare Metal vs. Drug-Eluting Stents Which One and When?
Stents are small mesh scaffolds deployed inside an artery to maintain its diameter after angioplasty. Bare metal stents provide structural support but carry a higher restenosis rate over time. Drug-eluting stents coated with medication to prevent cellular overgrowth offer improved long-term patency in selected arterial segments. Stents are not appropriate for every location: in arteries subject to significant movement and bending, such as the popliteal artery behind the knee, stent fracture is a risk, and alternative approaches may be preferred.
Atherectomy Removing Plaque Rather Than Just Pushing It Aside
Atherectomy devices physically remove plaque from inside the artery rather than compressing it. Several types are available directional, rotational, orbital, and laser atherectomy each suited to different plaque characteristics and locations. Atherectomy is particularly valuable in heavily calcified arteries where standard balloon angioplasty achieves suboptimal results, and in below-the-knee vessels supplying the foot in critical limb ischemia patients.
Combining Techniques Why Many Patients Benefit From More Than One Approach
In practice, most endovascular PAD procedures involve a combination of techniques tailored to the individual patient’s anatomy and disease pattern. Atherectomy followed by drug-coated balloon angioplasty, or balloon angioplasty with selective stenting at heavily calcified segments, often achieves better results than any single technique alone. The choice of approach is guided by pre-procedure imaging, intra-procedural assessment, and the operator’s experience.
Expected Patency and Long-Term Results How Long Does It Last?
What Is Arterial Patency and Why Does It Matter?
Arterial patency refers to whether a treated artery remains open and functional over time. Primary patency describes arteries that remain open without any further intervention. Secondary patency includes arteries that have been re-treated to restore flow. Patency rates vary depending on the location and extent of disease, the technique used, and the patient’s risk factor profile and they are one of the most important measures of endovascular treatment success.
Clinical Data on Long-Term Outcomes After Angioplasty and Stenting
Long-term patency data for endovascular PAD treatment has improved substantially with the adoption of drug-coated technologies. For superficial femoral artery disease one of the most commonly treated segments drug-coated balloon angioplasty achieves primary patency rates of approximately 70 to 80 percent at two years in suitable lesions. Below-the-knee interventions for critical limb ischemia focus less on patency and more on wound healing and limb salvage outcomes that are achieved in 70 to 85 percent of patients in specialist centres.
Lifestyle Changes That Protect Your Results and Slow Disease Progression
Endovascular treatment restores blood flow but it does not cure the underlying disease. Long-term results are strongly influenced by the patient’s commitment to risk factor modification. Smoking cessation is the single most impactful change a PAD patient can make. Antiplatelet medication, statin therapy, blood pressure and diabetes control, regular supervised exercise, and dietary improvement all play a critical role in maintaining the results of treatment and preventing disease progression in untreated arterial segments.
Can Angioplasty Help You Avoid Amputation?
Limb Salvage Rates With Endovascular Treatment What the Research Shows
The evidence supporting endovascular treatment as a limb-salvage strategy in critical limb ischemia is compelling. Large registries and multicentre trials consistently report limb salvage rates of 80 to 90 percent at one year following successful revascularisation in CLI patients. The key word is successful restoring adequate blood flow to the foot is the primary goal, and the more distal and complete the revascularisation, the better the wound healing outcomes. For patients facing amputation, an endovascular attempt at revascularisation is now considered the appropriate first step at most specialist vascular centres.
When Angioplasty Alone Is Not Enough Hybrid and Surgical Options
Endovascular treatment is not suitable for every patient or every pattern of disease. Long-segment occlusions, heavily calcified vessels with no suitable landing zones, and failed prior endovascular attempts may require surgical bypass or a hybrid approach combining open surgery with endovascular techniques in the same procedure. The decision between endovascular, hybrid, and open surgical treatment should be made by a multidisciplinary vascular team with access to all techniques, guided by the patient’s anatomy, fitness for surgery, and clinical urgency.
The Importance of Acting Before Critical Limb Ischemia Sets In
The single most important message in PAD management is this: do not wait. Claudication is treatable. Critical limb ischemia is an emergency. The earlier arterial disease is identified and treated, the greater the range of options available, the simpler the intervention required, and the better the long-term outcomes. Patients who present with established gangrene or extensive tissue loss face a far more complex treatment pathway and a higher risk of major amputation than those who seek help at the claudication stage.
Is Endovascular Treatment Right for You?
Key Questions to Ask Your Vascular Specialist
At your vascular consultation, consider asking:
- What is the severity of my arterial disease and which arteries are affected?
- Am I a candidate for angioplasty, drug-coated balloon treatment, or stenting?
- Would atherectomy improve my results given the characteristics of my blockage?
- What are the realistic expectations for symptom relief and patency in my case?
- What lifestyle changes should I make to protect my results long-term?
- How frequently will I need follow-up imaging after treatment?
- If endovascular treatment fails, what are the surgical options?
Atherectomy devices physically remove plaque from inside the artery rather than compressing it. Several types are available directional, rotational, orbital, and laser atherectomy each suited to different plaque characteristics and locations. Atherectomy is particularly valuable in heavily calcified arteries where standard balloon angioplasty achieves suboptimal results, and in below-the-knee vessels supplying the foot in critical limb ischemia patients.
What a Vascular Assessment and Angioplasty Consultation Looks Like
A vascular assessment for PAD begins with a detailed clinical history and physical examination, including pulse assessment and ankle-brachial index measurement. Duplex ultrasound maps the arteries of the leg non-invasively. CT angiography provides a detailed roadmap of the disease for procedure planning. From assessment to treatment, the process in most specialist centres takes one to three weeks with urgent cases expedited significantly faster.
Blocked leg arteries are serious but they are not a sentence to amputation. With modern endovascular tools, experienced vascular specialists, and early intervention, the majority of patients can have blood flow restored, symptoms relieved, and limbs saved. If you have leg pain, a non-healing wound, or risk factors for PAD, do not delay. A vascular consultation could change everything.