
Uterine Fibroid Embolization (UFE): The Non-Surgical Alternative to Hysterectomy
Introduction: Why More Women Are Choosing UFE Over Hysterectomy
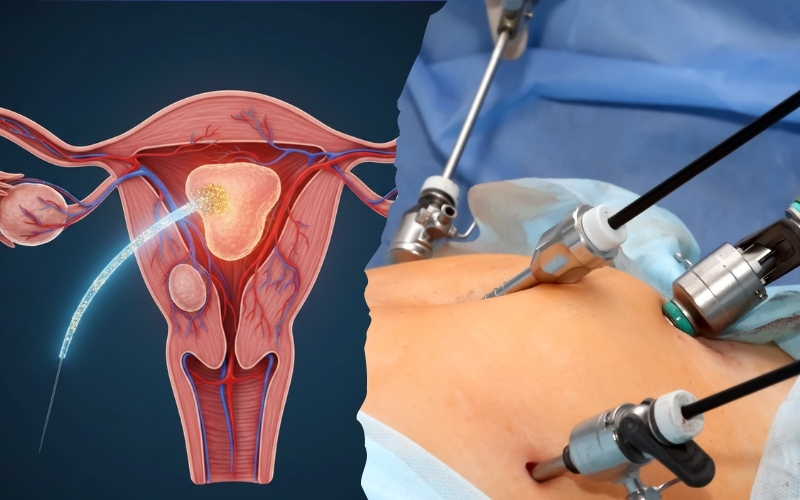
For decades, women suffering from uterine fibroids were offered a limited set of options endure the symptoms, take medication to manage them temporarily, or undergo a hysterectomy to remove the uterus entirely. Today, there is a fourth path. Uterine Fibroid Embolization (UFE) is a minimally invasive, clinically proven procedure that shrinks fibroids, relieves symptoms, and preserves the uterus without a single surgical incision.
What Are Uterine Fibroids and How Common Are They?
Uterine fibroids are non-cancerous growths that develop in or around the wall of the uterus. They are composed of muscle and fibrous tissue and can range in size from a small seed to a growth large enough to distort the shape of the uterus. Fibroids are remarkably common studies estimate that up to 70 to 80 percent of women will develop fibroids by the age of 50, though many never experience symptoms severe enough to require treatment.
The Problem With "Just Remove the Uterus" Why Surgery Isn't Always the Answer
Hysterectomy is a major surgical procedure with a significant recovery period, potential complications, and permanent consequences including the complete loss of fertility. For women who have not completed their families, who wish to preserve their uterus for personal or cultural reasons, or who are not suitable candidates for major surgery, hysterectomy is not an acceptable solution. UFE was developed precisely to fill this gap offering durable symptom relief without the need to remove the uterus.
Recognising the Symptoms: When Fibroids Start Affecting Your Life
Heavy Periods, Pelvic Pain, and Bloating The Classic Fibroid Symptoms
Not all fibroids cause symptoms, but when they do, the impact on daily life can be profound. The most common and disruptive symptoms include:
- Heavy or prolonged menstrual bleeding : Often severe enough to cause anaemia and fatigue
- Pelvic pressure or pain: A persistent feeling of heaviness or cramping in the lower abdomen
- Abdominal bloating : Fibroids can enlarge the uterus significantly, causing visible distension
- Painful periods: Cramping that is disproportionate and difficult to manage with standard pain relief
- Frequent urination: Large fibroids pressing on the bladder reduce its capacity
Less Obvious Signs of Fibroids Many Women Miss
Some fibroid symptoms are less immediately recognisable and are frequently attributed to other causes. These include lower back pain, pain during intercourse, constipation or difficulty with bowel movements, and leg pain caused by fibroids pressing on pelvic nerves. Unexplained iron-deficiency anaemia resulting from chronic heavy bleeding is another common but overlooked indicator.
When Symptoms Signal It's Time to Seek Help
If your periods regularly soak through protection, if pelvic pain is affecting your ability to work or socialise, or if you have been told you are anaemic without a clear explanation, it is time to seek a specialist evaluation. Fibroids do not resolve on their own and the earlier they are addressed, the more treatment options are available.
Who Is a Candidate for Uterine Fibroid Embolization?
The Ideal UFE Candidate: What Specialists Look For
UFE is suitable for most pre-menopausal women with symptomatic uterine fibroids who wish to avoid surgery and preserve their uterus. The ideal candidate has confirmed fibroid diagnosis on imaging, symptoms that are significantly impacting quality of life, no active pelvic infection, and no contraindications to the contrast dye used during the procedure. UFE can treat multiple fibroids of varying sizes simultaneously an advantage over surgical myomectomy, which may not address all fibroids in a single operation.
Who May Not Be Suitable for UFE and Why
UFE is not appropriate for all women. Those with pedunculated fibroids growths attached to the uterus by a thin stalk may not be suitable, as embolization can cause the fibroid to detach and create complications. Women with suspected or confirmed uterine or cervical cancer, active pelvic inflammatory disease, or severe contrast allergy require alternative management. Women with a strong desire to conceive should also have a detailed fertility discussion with their specialist before proceeding.
The Role of MRI and Ultrasound in Confirming Candidacy
Before UFE is recommended, detailed imaging is essential. Pelvic MRI is the gold standard it maps the number, size, location, and blood supply of each fibroid with precision, helping the interventional radiologist plan the procedure and predict outcomes. Ultrasound is often used as the initial screening tool. Together, these investigations confirm whether UFE is the most appropriate treatment and help set realistic expectations for results.
The UFE Procedure Explained: What Happens Step by Step
How UFE Works Cutting Off the Fibroid's Blood Supply
UFE works on a straightforward biological principle: fibroids depend entirely on their blood supply to survive and grow. By blocking that supply, the fibroid is starved of oxygen and nutrients causing it to shrink and die off over the following weeks and months. During the procedure, an interventional radiologist guides a thin catheter through a small puncture in the wrist or groin artery, navigates it to the uterine arteries under live X-ray guidance, and releases tiny particles called microspheres that block blood flow to the fibroids.
What to Expect on the Day of the Procedure
UFE is performed under conscious sedation or light general anaesthesia you are comfortable and relaxed throughout. The procedure takes approximately 60 to 90 minutes. The catheter access point is no larger than a small nick in the skin, requiring no stitches. After the procedure, patients are monitored for a few hours in a recovery area before being discharged typically on the same day or the following morning.
How Long Does UFE Take and Is It Painful?
The procedure itself is not painful thanks to sedation. After UFE, most women experience post-embolization syndrome cramping, mild fever, nausea, and fatigue in the first 24 to 48 hours as the body responds to the treated fibroids. This is a normal and expected part of the healing process, managed with prescribed pain relief and anti-inflammatory medication. It is temporary, and it is a sign that the procedure is working.
Recovery Timeline: What the First Days, Weeks, and Months Look Like
The First 24 to 48 Hours After UFE What Is Normal
The first two days following UFE are the most uncomfortable. Cramping, low-grade fever, fatigue, and nausea are common as the body processes the embolized fibroid tissue. Most women manage this at home with prescribed medication and rest. Keeping well-hydrated, eating lightly, and avoiding strenuous activity during this period helps the recovery proceed smoothly
Week One to Four: Managing Symptoms and Returning to Daily Life
By the end of the first week, most women feel significantly better and are able to return to light daily activities. Office-based work is often possible within seven to ten days. Physical exertion, heavy lifting, and sexual activity are typically restricted for two to four weeks. A vaginal discharge may be present for several weeks as fibroid tissue breaks down this is normal and expected.
Three to Six Months: Fibroid Shrinkage and Symptom Resolution
The full benefits of UFE develop gradually. Over three to six months, treated fibroids shrink by an average of 40 to 60 percent in volume. Heavy periods become lighter often returning to normal within the first two to three menstrual cycles. Pelvic pressure, bloating, and urinary frequency typically resolve in parallel with fibroid shrinkage. A follow-up MRI at three to six months confirms treatment success and the degree of shrinkage achieved.
UFE and Pregnancy: What Every Woman Should Know
Can You Get Pregnant After UFE? What the Research Shows
Pregnancy after UFE is possible, and a number of successful pregnancies have been reported in women who underwent the procedure. However, UFE is not currently recommended as a first-line treatment for women whose primary goal is future pregnancy. The procedure affects blood flow to the entire uterus not just the fibroids and there is evidence of a modest increase in the risk of premature delivery and miscarriage compared to surgical alternatives.
UFE vs. Myomectomy Which Is Better If You Want to Conceive?
For women who wish to preserve fertility, myomectomy surgical removal of the fibroids while leaving the uterus intact remains the preferred option. Myomectomy has a more established safety profile in the context of subsequent pregnancy. However, it carries its own surgical risks and may not address all fibroids if multiple are present. The right choice depends on the individual’s fibroid burden, age, overall health, and the strength of her desire to conceive.
Having an Honest Conversation With Your Specialist About Fertility
If you are considering UFE and have any plans certain or uncertain for future pregnancy, this must be a central part of your consultation. A good specialist will present all available options transparently, outline the evidence for each in the context of fertility, and support you in making a fully informed decision that aligns with your priorities and life plans.
Real Patient Outcomes: What Women Experience After UFE
Clinical Success Rates and Symptom Relief What the Data Says
UFE has an extensive evidence base built over more than 25 years of clinical use. Large-scale studies consistently report that 85 to 90 percent of women experience significant improvement in heavy bleeding following UFE, with comparable rates of improvement in pelvic pain, pressure, and urinary symptoms. These outcomes are durable and comparable to those achieved with hysterectomy without the surgical intervention.
Long-Term Results: Does UFE Last, or Do Fibroids Come Back?
The fibroids treated by UFE do not regrow once the blood supply is permanently blocked, those fibroids are gone. However, in a small percentage of women particularly younger women with a high fibroid burden new fibroids can develop over time from previously undetected seedling fibroids. Studies report that approximately 20 to 25 percent of women will require a further intervention within five years, compared to a re-intervention rate of zero following hysterectomy (since the uterus is removed). This trade-off is one women should understand before choosing UFE.
Patient Satisfaction Compared to Hysterectomy
Despite the possibility of retreatment, patient satisfaction following UFE is consistently high. Women report relief from debilitating symptoms, preservation of their uterus, rapid return to normal life, and avoidance of major surgery as significant positives. Comparative studies show UFE satisfaction rates broadly equivalent to hysterectomy with the added benefits of shorter recovery, lower procedural risk, and uterine preservation.
UFE vs. Hysterectomy: A Side-by-Side Comparison
Recovery Time, Hospital Stay, and Return to Normal Life
|
#
|
UFE
|
Hysterectomy
|
|---|---|---|
|
Procedure Type
|
Minimally Invasive
|
Major Surgery
|
|
Hospital Stay
|
Same day/ overnight 2 to 5 days
|
2-5 days
|
|
Return to Work
|
7 to 10 days
|
4-8 weeks
|
|
General anaesthesia
|
Usually not required
|
Required
|
|
Uterus preserved
|
Yes
|
No
|
|
Fertility Preserved
|
Possibly
|
No
|
|
Fibroid Recurrence
|
Small risk
|
None
|
Preserving the Uterus Why It Matters Beyond Fertility
For many women, preserving the uterus is important for reasons beyond the ability to conceive. The uterus plays a role in pelvic support and some research suggests hormonal and sexual function. For women who feel strongly about keeping their uterus intact for personal, cultural, or psychological reasons, UFE provides a medically sound pathway to symptom relief without compromise.
Is UFE the Right Choice for You?
Key Questions to Ask Your Interventional Radiologist
At your UFE consultation, consider asking:
- Am I a good candidate for UFE based on my fibroid type, size, and location?
- How many UFE procedures has your team performed, and what are your outcomes?
- What are the realistic expectations for symptom relief in my case?
- What is the likelihood I may need further treatment in the future?
- How does UFE compare to myomectomy for my specific situation?
- What monitoring will I need after the procedure?
Taking the First Step - What a UFE Consultation Looks Like
A UFE consultation begins with a thorough review of your symptoms, medical history, and existing imaging. If you have not yet had a pelvic MRI, your specialist will arrange one. From there, your suitability for the procedure is assessed, treatment options are discussed in full, and if UFE is right for you a procedure date is scheduled. The entire process from first consultation to completed treatment typically takes two to four weeks.
You do not have to choose between suffering and major surgery. UFE offers a third path proven, precise, and preserving. Speak to a specialist and find out if it is right for you.